
Lumbopelvic hip complex dysfunction also referred to as lower cross syndrome, describes
Muscular issues can work their way up the kinetic chain, which is a fancy way of saying: what happens in one area of the body can cause issues in other areas. Whether it be forward head posture or upper crossed syndrome we usually see many of these dysfunctional patterns coincide with one another.
There are various lower body muscle imbalances that can exist, and there are conditions opposite to LPHCD as well. Performing an assessment is important to determine what muscles are actually dysfunctional.
What is a muscle imbalance?
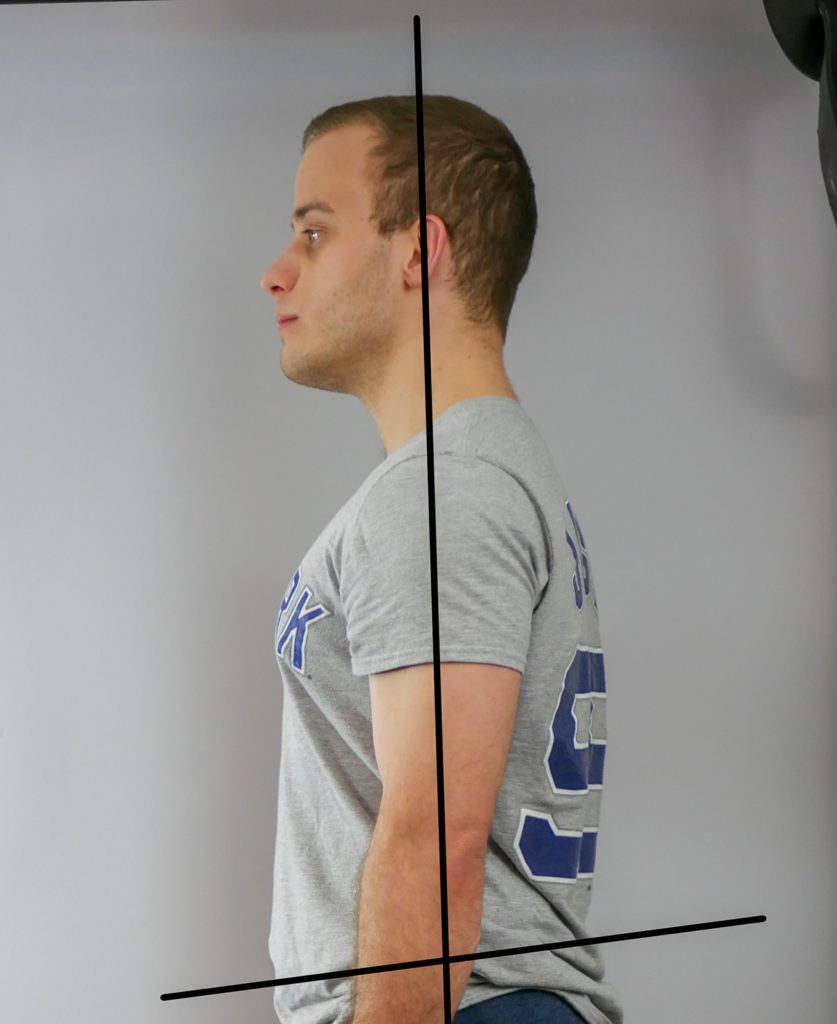
Optimal alignment 
Excessively rounded lower back, forward weight shift indicates Lower Crossed Syndrome.
A muscle imbalance is when the muscles surrounding a joint stop functioning properly. Muscles operate your joints in force couples. A force couple consists of opposite muscles. A good example of a force couple is at the elbow. The biceps control elbow flexion, the triceps perform the opposite motion, elbow extension.
If one of the muscles in a force couple becomes overused and overdeveloped, the opposite tends to become weakened and the force couple will negatively affect joint function.
How does a muscle imbalance happen?
Muscle imbalances occur when we have certain muscles being used or overused and overdeveloped. Conversely, we have muscles that become weakened and require strengthening. This is an oversimplification. There are many variables that can lead to muscular imbalances, such as over-exercising certain muscle groups, or sitting all day at work, and favoring one side while carrying something like a bag over one shoulder.
The common approach for repairing muscle imbalances involves identifying these overused muscles that have become dominant, aka overactive, and performing mobility techniques such as foam rolling, and possibly stretching and dynamic stretching (stretching is debated and the mechanism is unclear).
Strengthening the underactive muscles, which generally perform opposite functions of the overactive muscles, is
What muscles are involved?
Let’s go over the muscles that tend to be overactive and underactive in lower crossed syndrome. We can also consult a solutions table to give us a solid reference for key players in lower body muscle imbalances.
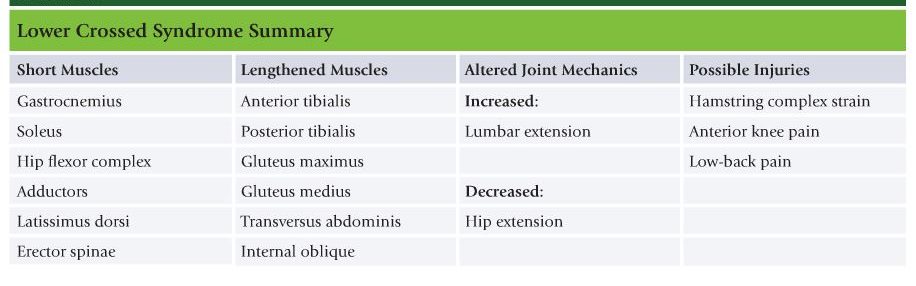
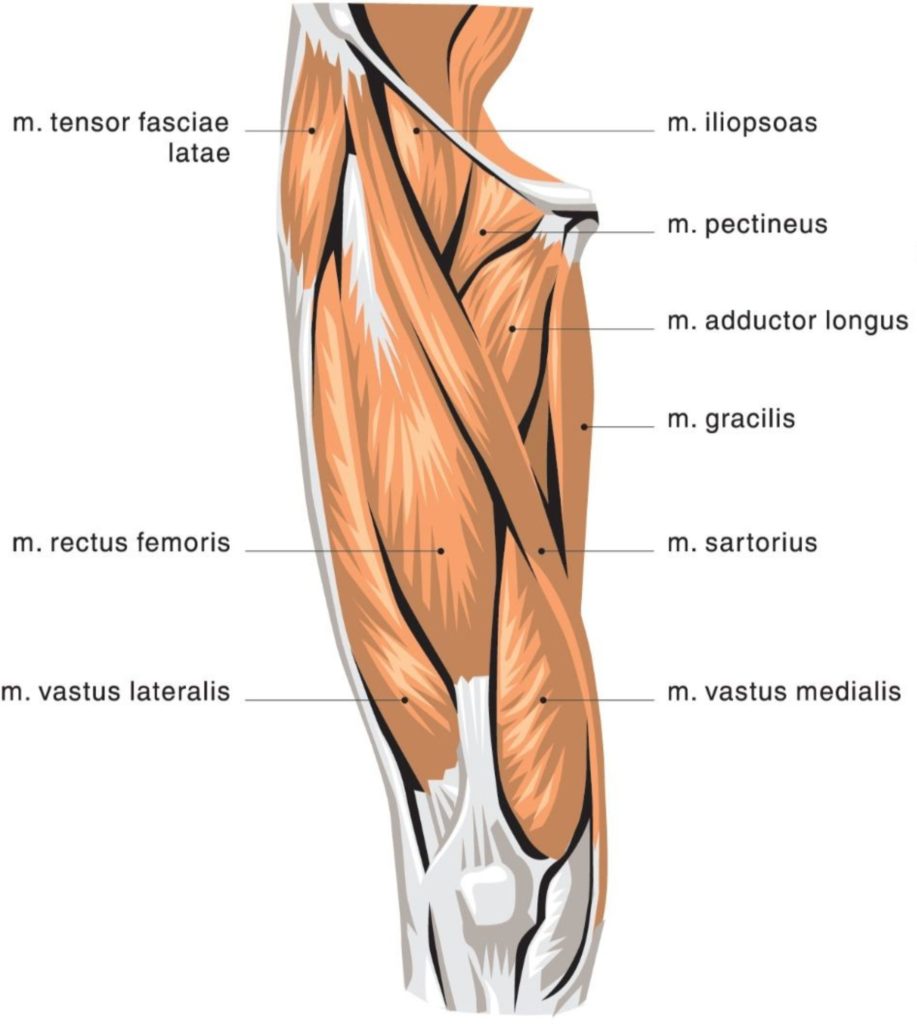
Overactive muscles in lower crossed syndrome:
The hip flexor complex (psoas, rectus femoris, tensor fascia
Latissimus dorsi, erector spinae – These are your back muscles and lower back stabilizers. The erectors directly flex your lower back and cause it to curve. The lat’s main function is to bring your arm back down towards the body, but the lats also play an important role in keeping your pelvis stable while your glute performs locomotion, moving you around.
Gastrocnemius, soleus – These are your calf muscles. They plantar flex your foot (point the toes down). They tend to effect knee extension and cause problems in conjunction with other muscles in lower crossed syndrome. They are also key players in pronation distortion
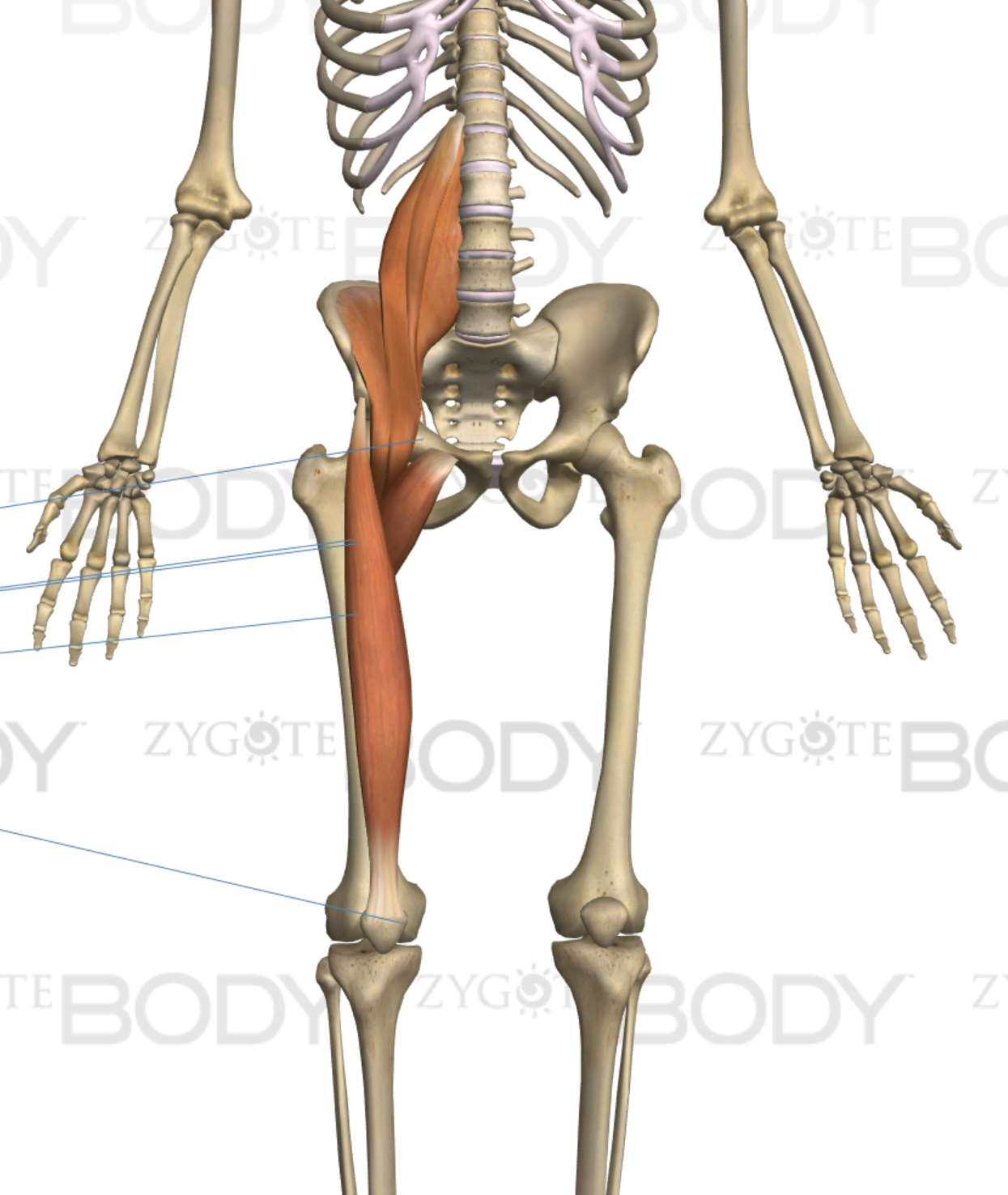
Hip Flexors 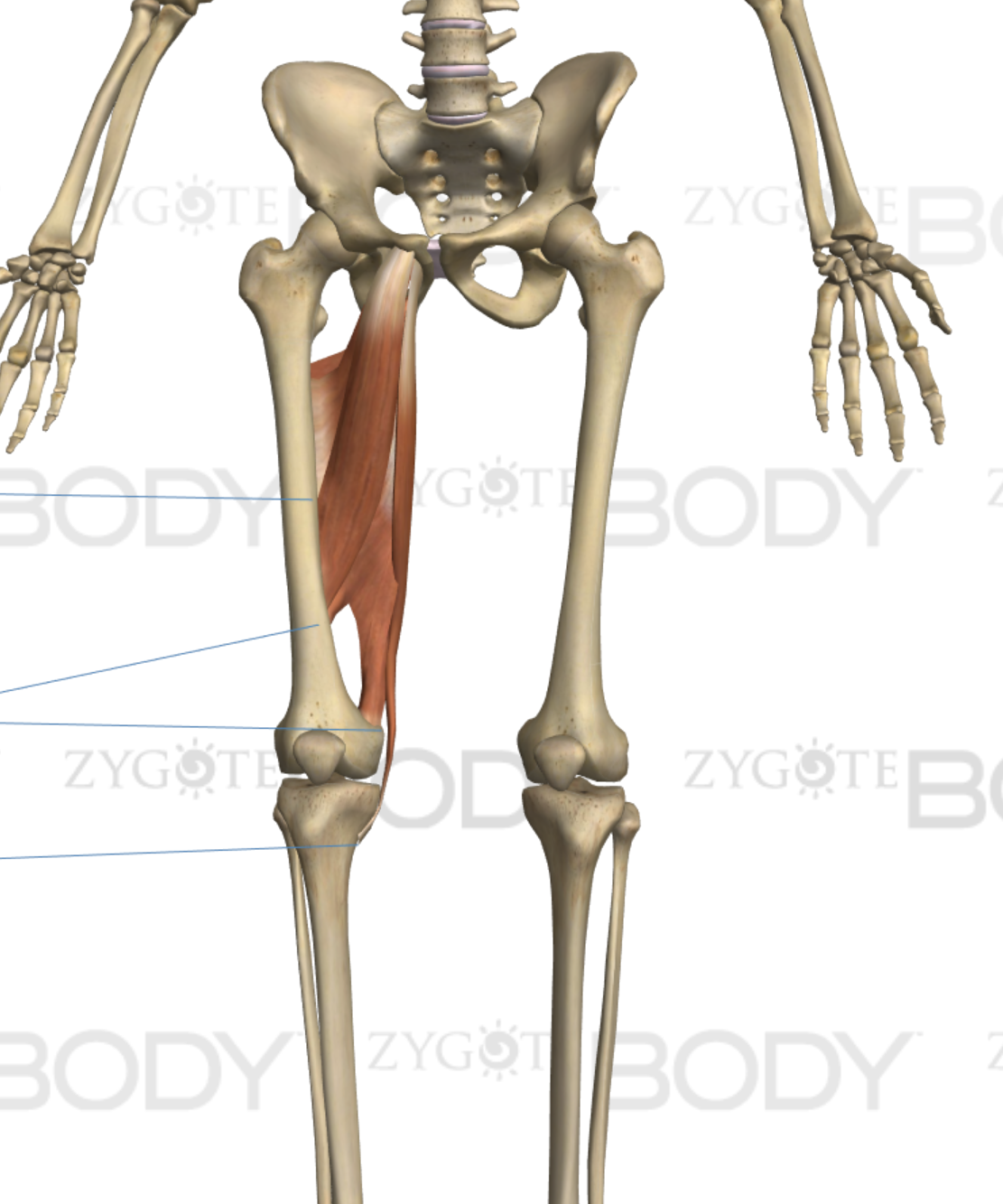
Adductors 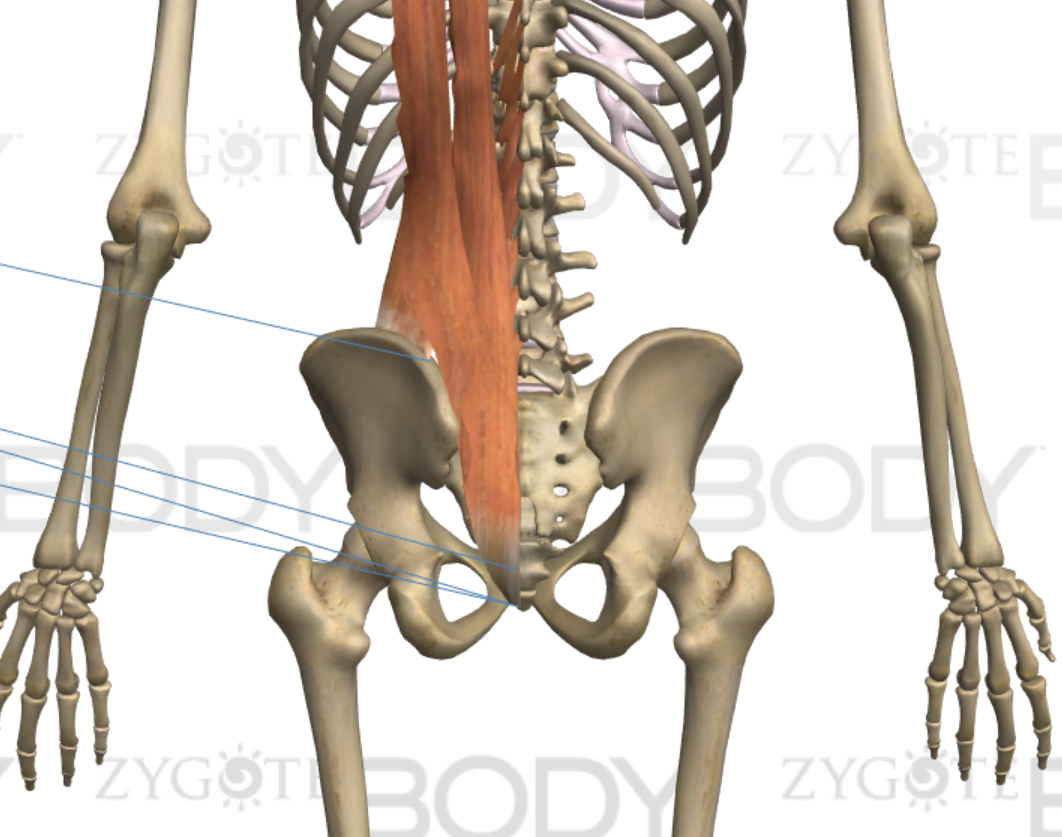
Lower back erectors 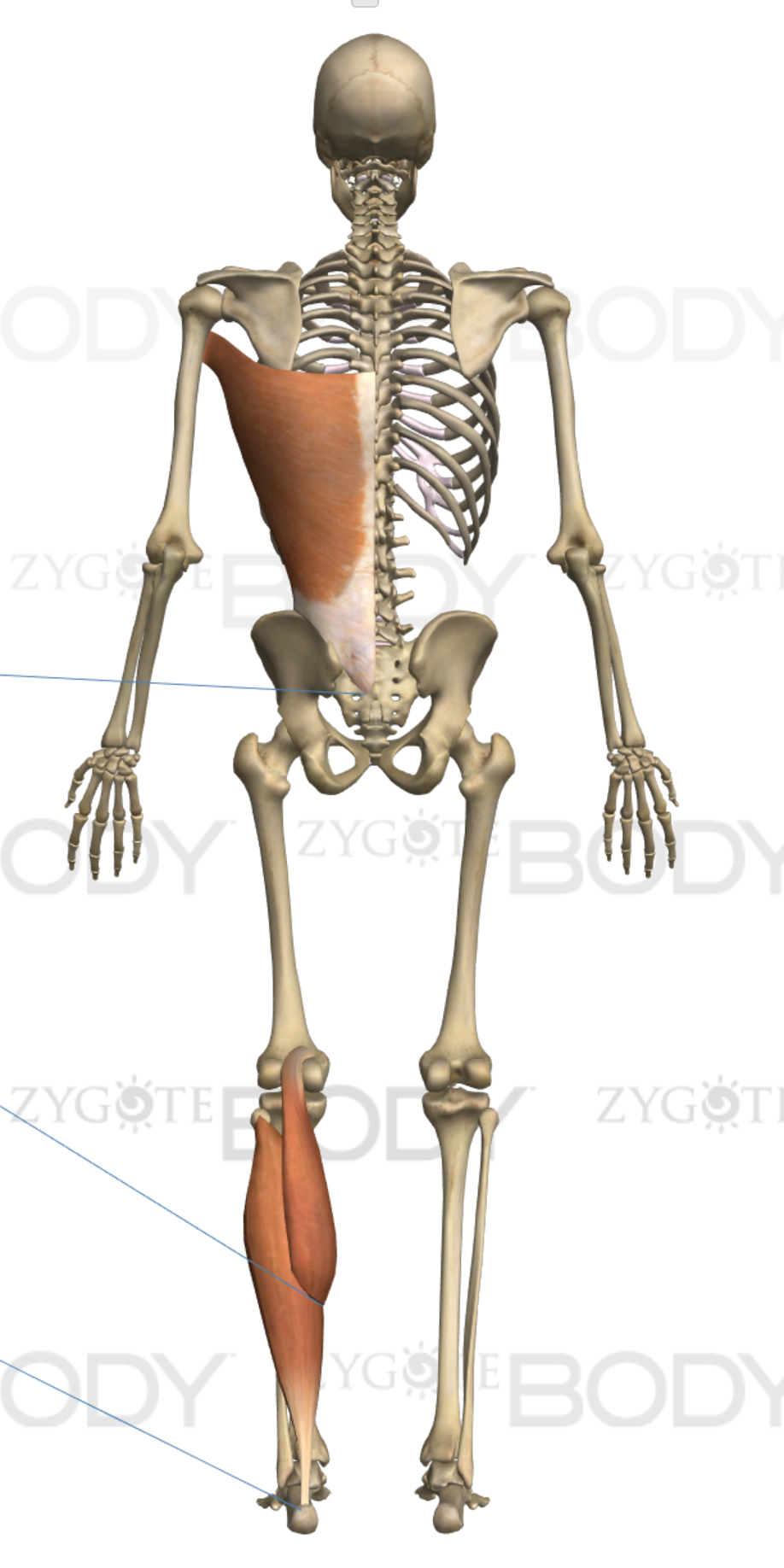
Lats and Calf
Underactive muscles in lower crossed syndrome:
The under-active lengthened, and weak muscles include (but are not limited to) the gluteus maximus, gluteus medius, transverse abdominis, internal oblique, anterior tibialis, posterior tibialis. These are your butt muscles, your core, and your shin muscles!
The glute and hamstring dynamic
People’s glutes tend to shut off and become inhibited. Our glutes are designed to extend our legs behind us and are the main functional muscle for walking and locomotion. If our glutes aren’t functioning properly our hamstrings tend to pick up the slack. Our hamstrings become dominant in this example. Hamstrings often “Feel tight” but this can be misleading. It is very likely that by stretching your hip flexors and activating your glutes, your hamstrings will feel relief. It is because of this that many physical therapists don’t recommend hamstring stretches like the first form of treatment.
The thing is, many people assume stretching anything is beneficial, and the hamstring stretches are a very standard go to in gym class, or before activity, on the field for many sports, etc. It’s important that we don’t stretch muscles that could be weakened or lengthened, as this tends to feed into issues. It’s also important that we don’t continue to strengthen muscles that might be overdeveloped and contributing to a problem. We must utilize assessments to determine if we really have a hip imbalance before performing corrective exercise!
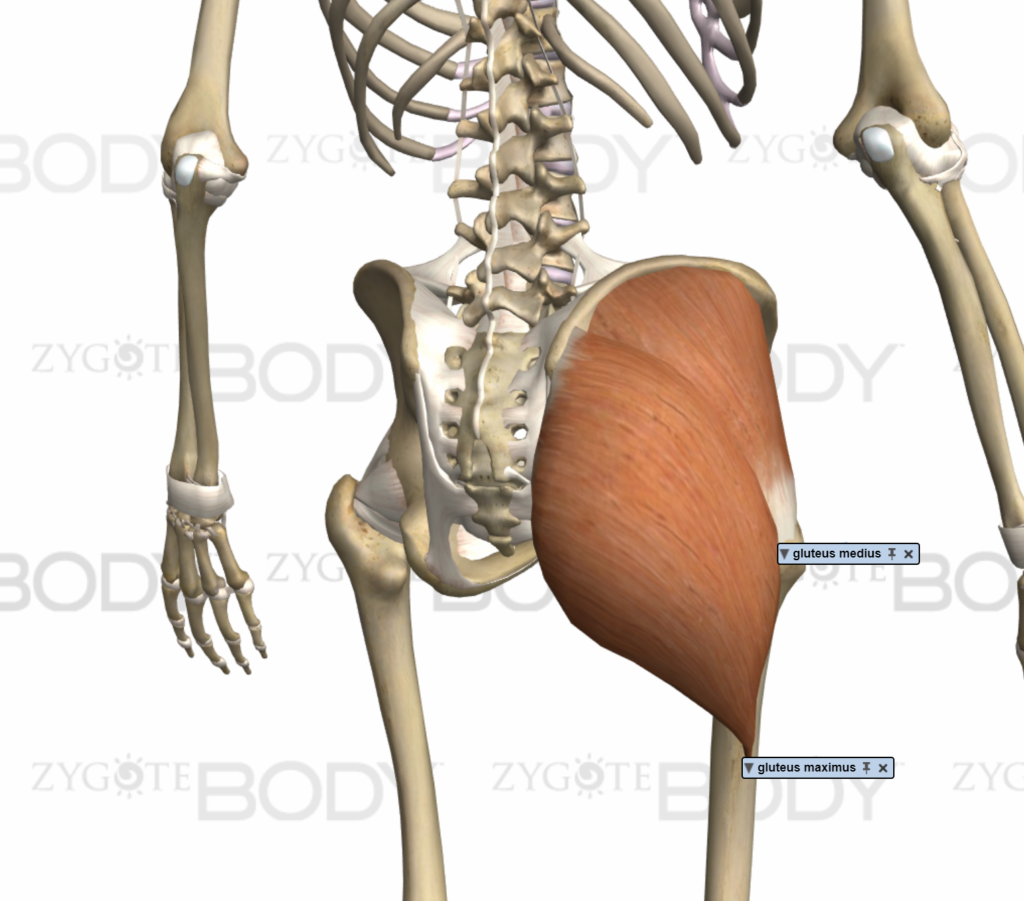
Glutes 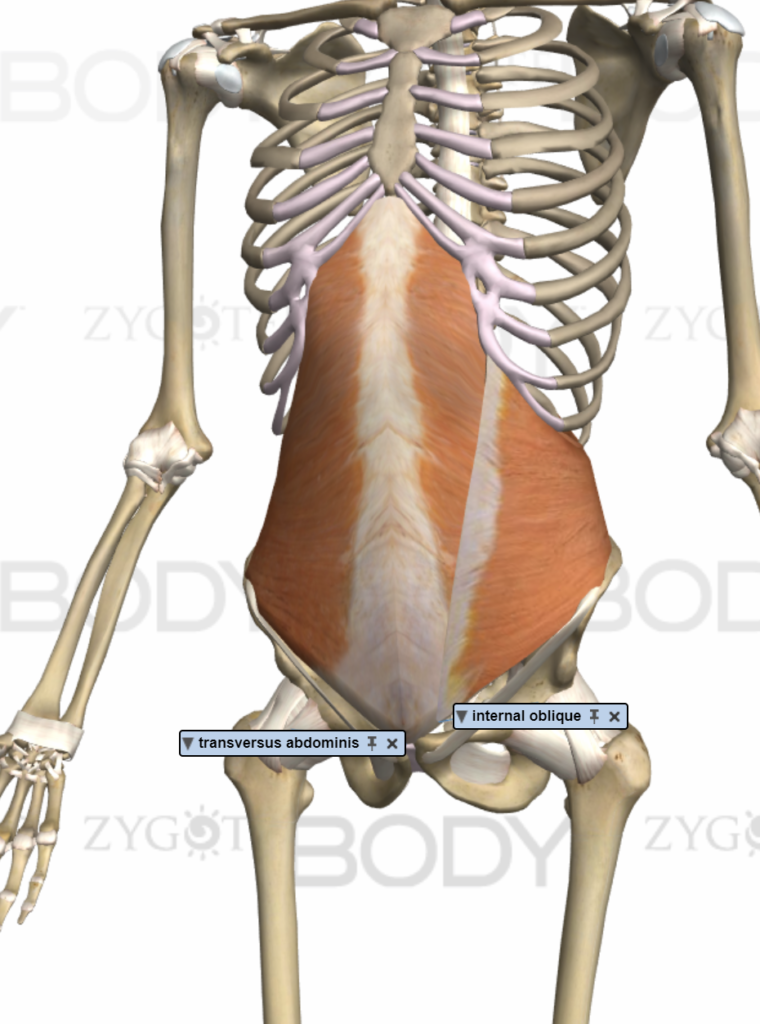
Core muscles
Do you have it?
With a muscle imbalance, it is important to understand that unless we address the over-activity of contributing muscles like the hip flexors, it becomes difficult to activate and strengthen the opposite muscles.
Performing an assessment is key. One of the best assessments for lower body dysfunction is the overhead squat assessment. The overhead squat assessment can help to reveal what muscle groups are really affecting your pelvic positioning.
Now what?
Consult the Lower Crossed Syndrome Corrective Exercises page for techniques to begin to correct this dysfunction!